Traduction: G.M.
The Need for Objective Measures of Stress in Autism
Front. Psychol., 27 January 2017
| https://doi.org/10.3389/fpsyg.2017.00064
 Cédric Hufnagel1,
Cédric Hufnagel1,  Patrick Chambres1,
Patrick Chambres1,  Pierre R. Bertrand2 and
Pierre R. Bertrand2 and  Frédéric Dutheil1,3,4*
Frédéric Dutheil1,3,4*- 1CNRS, LaPSCo, Stress Physiologique et Psychosocial, Université Clermont Auvergne, Clermont-Ferrand, France
- 2CNRS, LMBP, Université Clermont Auvergne, Clermont-Ferrand, France
- 3Preventive and Occupational Medicine, University Hospital of Clermont-Ferrand (CHU), Clermont-Ferrand, France
- 4Faculty of Health, Australian Catholic University, Melbourne, VIC, Australia
Impact physiologique et psychologique des facteurs de stress
En dépit de la définition multiple du stress, le sens du stress peut se référer aux réponses comportementales ou mentales adaptatives qui sont prêtes à traiter les conséquences de la vie courante des facteurs de stress, comme une attention accrue pour accomplir une tâche exigeante sur le plan mental. Le stress peut être réel ou perçu, agréable ou désagréable (Woda et al., 2016). Une adaptation permanente aux facteurs stressants quotidiens est nécessaire, via le système de stress physiologique. La réponse physiologique au stress déclenche des adaptations métaboliques aux facteurs de stress aigus (via l'activation du système nerveux autonome qui entraîne principalement la libération d'épinéphrine par la médullosurrénale) et anticipe ce qui peut arriver (via l'activation de l'axe hypothalamo-hypophysaire surrénalien entraînant la libération de corticostéroïdes Par la moelle corticale) (McEwen, 2000, Woda et al., 2016). Des conséquences morbides peuvent être attendues lorsqu'un individu est affecté par une défaillance du système de réponse au stress à des facteurs de stress. Par conséquent, dans son lieu commun, le terme «stress» est souvent considéré comme un concept négatif, avec des conséquences morbides (Woda et al., 2016). L'un de ces effets négatifs est l'anxiété. Avec l'anxiété, la peur surmonte toutes les émotions et s'accompagne d'inquiétude et d'appréhension (Sylvers et al., 2011; Adhikari, 2014). Bien qu'il existe un chevauchement définitif entre le stress et l'anxiété, nous utiliserons le terme stress comme effet physiologique et psychologique négatif des facteurs de stress.Physiological and Psychological Impact of Stressor
Despite the numerous definition of stress, the meaning of stress could refer to the adaptive behavioral or mental responses willing to address the common life consequences of stressors, such as increased attention to perform a mentally demanding task. The stressor can be real or perceived, pleasant, or unpleasant (Woda et al., 2016). Permanent adaptation to normal daily stressors is needed, via the physiological stress system. The physiological stress response triggers metabolic adaptations to the acute stressors (via activation of the autonomic nervous system mostly resulting in release of epinephrine by the adrenal medulla) and anticipates what may happen (via activation of the hypothalamo-pituitary adrenal axis resulting in release of corticosteroids by the cortical medulla) (McEwen, 2000; Woda et al., 2016). Morbid consequences can be expected when an individual is affected by a failure of the stress response system to stressors. Therefore, in its commonplace, the term “stress” is often viewed as a negative concept, with morbid consequences (Woda et al., 2016). One of these negative effects is anxiety. With anxiety, fear overcomes all emotions and is accompanied by worry and apprehension (Sylvers et al., 2011; Adhikari, 2014). While there is a definite overlap between stress and anxiety, we will use the term stress as a negative physiological and psychological impact of stressors.Stress dans l'autisme
Les personnes avec trouble du spectre de l'autisme ont souvent des difficultés de communication et d'interaction sociale résultant d'un traitement de l'information atypique et d'anomalies dans l'intégration sensorielle. Cela provoque un état de surcharge cognitive et émotionnelle associé à un stress accru, par l'implication du système nerveux autonome, qui peut conduire à l'apparition d'un comportement social inapproprié. Cependant, dans la plupart des publications actuelles (Reaven et al., 2012, Corbett et al., 2016, Bishop-Fitzpatrick et al., 2017), le stress des personnes avec trouble du spectre de l'autisme est évalué par des questionnaires ou parfois par des biomarqueurs salivaires. Malgré le manque de cohérence entre les scores aux questionnaires et les niveaux de biomarqueurs salivaires (Corbett et al., 2009 et Spratt et al., 2012), ce n'est pas une évaluation directe et continue. Cela suppose que les soignants ou les personnes autistes soient en mesure de reconnaître les symptômes externes et internes du stress, mais aussi que le stress déclenche systématiquement une réponse comportementale identifiable ou observable. Nous croyons que l'évaluation du stress ne doit pas être subjective. Les personnes avec trouble du spectre de l'autisme devraient bénéficier de mesures objectives et continues du stress, en particulier sachant que près de la moitié des personnes avec autisme n'ont pas accès à une communication efficace pour exprimer ce stress interne (American Psychiatric Association, 2013).Stress in Autism
People with autism spectrum disorder often have
difficulties in communication and social interaction resulting from
atypical information processing and abnormalities in sensory
integration. This causes a cognitive and emotional overload state
associated with an increased stress, by the involvement of the autonomic
nervous system, that can lead to the appearance of inappropriate social
behavior. However, in most actual publications (Reaven et al., 2012; Corbett et al., 2016; Bishop-Fitzpatrick et al., 2017),
the stress of individuals with autism spectrum disorder is evaluated by
questionnaires or sometimes by saliva biomarkers. Despite the lack of
consistency between scores to questionnaires and levels of saliva
biomarkers (Corbett et al., 2009; Spratt et al., 2012),
they are not a direct and continuous assessment. This presupposes that
caregivers or people with autism are able to recognize external and
internal symptoms of stress, but also that stress systematically
triggers an identifiable or observable behavioral response. We believe
that stress evaluation should not be subjective. Individuals with autism
spectrum disorder should benefit from objective continuous measures of
stress, especially knowing that almost half of individuals with autism
do not have access to effective communication to express this inner
stress (American Psychiatric Association, 2013).
Biomarqueurs du stress
Aujourd'hui, la majeure partie de l'évaluation du stress est faite avec des biomarqueurs salivaires tels que le cortisol ou le déhydroépiandrostérone (DHEA), ou sa forme sulfatée (DHEA-S) (Danhof-Pont et al., 2011; Cependant, ces biomarqueurs ne donnent pas une évaluation directe et instantanée du stress ou de l'anxiété. Ils doivent être transportés dans un endroit frais pour être évalués dans un laboratoire spécialisé. Les niveaux de ces biomarqueurs reflètent un niveau de stress qui peut varier de quelques minutes à plusieurs heures, en fonction de leur demi-vie. Par exemple, le cortisol a une demi-vie courte de 20 minutes, et peut donc révéler un stress aigu; Tandis que la DHEA-S a une longue demi-vie de 16 h et révèle ainsi le stress global d'une longue période (une demi-journée) (Woda et al., 2016). En outre, les niveaux de DHEA-S auront besoin d'une longue période de temps (plusieurs demi-vie) pour revenir aux valeurs de base. Par conséquent, la DHEA-S est un biomarqueur du stress chronique. En outre, les biomarqueurs putatifs de stress qui ont besoin d'échantillon de sang sont exclus en raison de la faisabilité. Même si l'on ne tient pas compte du coût élevé de ces biomarqueurs, on note aussi un manque de spécificité et des résultats contradictoires (Oliveira et al., 2013, Fancourt et al., 2015, Hawn et al., 2015, Qi et al, 2016).Biomarkers of Stress
Today most of stress assessment is done with saliva
biomarkers such as cortisol or dehydroepiandrosterone (DHEA) levels, or
its sulfated form (DHEA-S) (Danhof-Pont et al., 2011; Lac et al., 2012).
However, those biomarkers do not give a direct and instantaneous
assessment of stress or anxiety. They need to be transported in a cool
storage for assessment in a dedicated laboratory. The levels of those
biomarkers reflect a level of stress which may vary from some minutes
ago to several hours ago, depending on their half-life. For example
cortisol has a short half-life of 20 min, and thus may reveal acute
stress; whereas DHEA-S has a long half-life of 16 h and thus reveals the
global stress of a long period (half a day) (Woda et al., 2016).
Moreover, DHEA-S levels will need a long period of time (several
half-life) to return to basal values. Therefore, DHEA-S is a biomarker
of chronic stress. Besides, putative biomarkers of stress which need
blood sample are excluded because of feasibility. Even if we do not
consider the high cost of those biomarkers, they also lack of
specificity and conflicting results are reported (Oliveira et al., 2013; Fancourt et al., 2015; Hawn et al., 2015; Qi et al., 2016).
La nécessité d'une surveillance continue du stress
La détection en temps réel du stress nécessite une surveillance continue. Pour évaluer le stress dans la vie quotidienne, nous avons également besoin d'appareils portables. Ces dispositifs doivent être non invasifs et sans douleur. Pour ces raisons, tous les marqueurs historiques de stress mesurés dans le sang, la salive ou l'urine sont exclus. La nécessité de s'adapter aux événements externes et internes implique l'activation du système nerveux autonome, qui est un équilibre entre l'activité sympathique et parasympathique (Shaffer et al., 2014). Le tonus vagal est considéré comme une mesure de l'activité parasympathique qui contrôle l'état de repos des organes internes via le nerf vague. La mesure la plus précise du tonus vagal est fournie par son effet sur la fréquence cardiaque. Le contrôle vagal du coeur induit une augmentation de la variabilité du rythme cardiaque (VRC) (Park et Thayer, 2014, Scott et Weems, 2014). La VRC est la variation entre deux battements consécutifs: plus la variation est élevée, plus l'activité parasympathique est élevée. Une VRC élevée reflète le fait qu'un individu peut s'adapter en permanence aux changements micro-environnementaux. Une surcharge de contrainte induit une diminution de la VRC et les mécanismes d'adaptation sont dépassés. Par conséquent, la faible VRC est à la fois un marqueur du risque cardiovasculaire et un biomarqueur du stress (Dutheil et al., 2012; Boudet et al., 2017). Pratiquement, la mesure de la VRC est facile, non intrusive et sans douleur, et assure une surveillance continue de l'activité du système nerveux autonome.The Need for a Continuous Monitoring of Stress
Real-time detection of stress needs continuous
monitoring. To assess stress in daily life, we also need portable
device. These devices must be non-invasive and pain-free. For these
reasons, all historical markers of stress measured in blood, saliva, or
urine, are excluded. The need to adapt to external and internal events
involve the activation of the autonomous nervous system, which is a
balance between sympathetic and parasympathetic activity (Shaffer et al., 2014).
Vagal tone is considered to be a measure of parasympathetic activity
which controls the resting state of internal organs via the vagus nerve.
The most precise measure of the vagal tone is provided via its effect
on heart rate. The vagal control of heart induces an increased heart
rate variability (HRV) (Park and Thayer, 2014; Scott and Weems, 2014).
HRV is the variation between two consecutive beats: the higher the
variation, the higher the parasympathetic activity. A high HRV reflects
the fact that an individual can constantly adapt to micro-environmental
changes. An overload of stress induces a decrease in HRV and the
adaptation mechanisms are exceeded. Therefore, low HRV is both a marker
of cardiovascular risk and a biomarker of stress (Dutheil et al., 2012; Boudet et al., 2017).
Conveniently, the measurement of HRV is easy, non-intrusive and
pain-free, and provides continuous monitoring of the activity of the
autonomic nervous system.
Mesure de la variabilité du rythme cardiaque
Le moyen le plus précis de mesurer la VRC est d'utiliser un Holter-électrocardiogramme qui est un petit dispositif médical appliqué sur la poitrine. Un Holter-électrocardiogramme donne le temps exact en millisecondes entre deux battements consécutifs, basé sur les ondes R (Malik et al., 1996). Le Holter-électrocardiogramme est cher, doit être placé avec précision, et peut causer un certain inconfort à l'usure. Par conséquent, les ceintures émetteurs de fréquence cardiaque proposent maintenant une mesure fiable de la VRC (Akintola et al., 2016, Hernando et al., 2016). En raison de la quantité importante de données à traiter, le VRC nécessite une analyse hors ligne qui n'est pas compatible avec l'évaluation en temps réel du stress. Une nouvelle méthode de développement qui utilise la détection de changements abrupts dans la VRC permettra d'identifier les événements stressants (Azzaoui et al., 2014, Dutheil et al., 2015). La fréquence cardiaque, et donc la VRC, sont l'une des mesures physiologiques les plus faciles d'accès au grand public. Une ceinture émettrice de fréquence cardiaque est une option de budget avec des mesures précises, mais pas aussi pratique et encore plus obstructive qu'un simple bracelet de poignet. Certains capteurs à poignet sont disponibles, mais manque de résolution pour être utilisés.Measuring Heart Rate Variability
The most accurate way of proceeding HRV is to use a
Holter-electrocardiogram which is a small medical device applied on the
chest. A Holter-electrocardiogram give the exact time in milliseconds
between two consecutive beats, based on R waves (Malik et al., 1996).
The Holter-electrocardiogram is expensive, need to be precisely placed,
and can cause some discomfort to wear. Therefore, heart rate
transmitter belts now propose reliable measure of HRV (Akintola et al., 2016; Hernando et al., 2016).
Due to the important amount of data to be processed, HRV require
offline analysis witch is not compatible with real-time evaluation of
stress. New method in development, that use detection of abrupt changes
in HRV, will allow the identification of stressful events (Azzaoui et al., 2014; Dutheil et al., 2015).
Heart rate, and thus HRV, are one of the easiest physiological
measurements accessible to the general public. A heart rate transmitter
belt is a budget option with accurate measures, but not as practical as
and still more obtrusive than a simple wrist-band. Some wrist-based
sensors are available but still lack of resolution to be used.
La détection de changements brusques
La littérature antérieure a rapporté une VRC basale normale ou déficiente chez les personnes avec trouble du spectre de l'autisme (Cheshire, 2012; Kushki et al., 2014). De même, même si les personnes autistes et de témoins sans autisme peuvent partager un modèle semblable de modifications autonomes suite à un stress mental aigu (Kushki et al., 2014), certains auteurs ont également signalé une réponse de la VRC émoussée à un stress aigu (Hollocks et al., 2014 , 2016). Malgré les réponses toujours liées au stress, les méthodes d'analyse de la réponse du VRC sont discutables. L'enregistrement électrocardiographique est typiquement segmenté en blocs a priori de 5 min chacun ou dans une autre période de temps fixe a priori. Notre méthode de point de changement est statistiquement différente. Nous détectons le changement abrupt, puis nous calculons la valeur moyenne de VFC entre deux changements abrupts consécutifs (figure 1). La détection de changements abrupts est une approche statistique basée sur une base individuelle et non sur un niveau normalisé de la population. Il n'est pas nécessaire d'avoir un groupe témoin. Les statistiques personnalisées sont calculées dans la série chronologique de chaque individu, excluant le biais. La détection des changements abrupts a une courte histoire en médecine, mais une longue histoire en finance quantitative, qui a conduit à plusieurs prix Nobel (Mandelbrot, 1963, Engle et Granger, 1982, Hansen, 1982, Granger, 2004).The Detection of Abrupt Changes
Previous literature have reported either normal or impaired baseline HRV in people with autism spectrum disorder (Cheshire, 2012; Kushki et al., 2014).
Similarly, even if people with autism and healthy controls may share
similar pattern of autonomic modifications following an acute mental
stress (Kushki et al., 2014), some authors also reported a blunted HRV response to an acute stress (Hollocks et al., 2014, 2016).
Despite the responses were still linked with stress, methods to analyze
HRV response are questionable. Electrocardiogram recording are
typically segmented into a priori blocks of 5 min each or other a priori
fixed period of time. Our change point method is statistically
different. We detect the abrupt change, then we calculate the mean value
of HRV between two consecutive abrupt changes (Figure 1).
The detection of abrupt changes is a statistical approach based on an
individual basis and not on a population normalized level. There is no
need for a control group. Personalized statistics are computed within
the time-series of each individual, precluding bias. Detection of abrupt
changes has a short history in medicine but a long history in
quantitative finance, which has led to several Nobel prizes (Mandelbrot, 1963; Engle and Granger, 1982; Hansen, 1982; Granger, 2004).
FIGURE 1
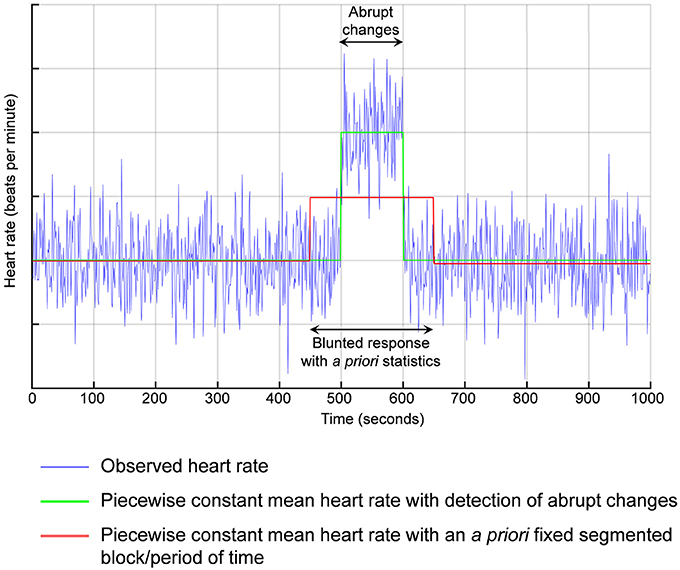
Figure 1. Détection de changements abrupts. Par exemple, si la réponse en fréquence cardiaque est retardée par rapport à la contrainte aiguë, les méthodes antérieures utilisant des périodes de temps a priori segmentées seraient en moyenne entre les valeurs de base et la réaction de stress conduisant à une réponse émoussée.
Figure 1. Detection of abrupt changes. For example, if the response in heart rate is delayed from the acute stress, previous methods using a priori segmented periods of time would average between the basal values and the stress reaction leading to a blunted response.
Évaluation du stress dans la vie quotidienne
Cependant, la plupart des études qui ont évalué la VRC chez les personnes autistes étaient en laboratoire et non dans la vie quotidienne réelle. Être en laboratoire est une tâche difficile pour les personnes avec trouble du spectre de l'autisme et peut engendrer une hyperréactivité du système nerveux autonome (Van Steensel et al., 2011; Jurko et al., 2016). De récents développements en matière de portabilité des appareils et de traitement des données permettent de concevoir de nouveaux dispositifs pouvant être utilisés dans la vie quotidienne pour effectuer l'évaluation du stress (El Kaliouby et al., 2006; Bientôt, juste une montre devrait fournir une surveillance fiable et continue de la VRC . Ces montres pourraient facilement être connectées à une application smartphone conçue pour la détection en ligne de changements brusques. Ces solutions innovatrices de traitement des données permettront d'avoir une vision réelle des niveaux de stress à fournir aux personnes avec un trouble du spectre de l'autisme et à leurs aidants naturels. En fin de compte, cette connaissance devrait permettre une intervention appropriée, en particulier par l'enseignement des auto-réponses dans différents contextes sociaux, limitant ainsi l'apparition de comportements perturbateurs (Dawson, 2008). Les possibilités ne sont pas limitées aux troubles du spectre de l'autisme et de nombreuses conditions ou situations de travail devraient bénéficier de mesures objectives du stress.Stress Assessment in Daily Life
However, most studies which evaluated HRV on individuals
with autism were in laboratory and not in real daily life. Being in a
laboratory is a challenging task by itself for people with autism
spectrum disorder, and can generate hyper-reactivity of the autonomic
nervous system (van Steensel et al., 2011; Jurko et al., 2016).
Recent development in device portability, as well as data processing,
give the opportunity to conceive new devices that can be used in daily
life to perform stress assessment (El Kaliouby et al., 2006; Picard, 2009).
Soon, just a watch should provide reliable continuous HRV monitoring.
These watches could easily be connected to a smartphone application
designed for the online detection of abrupt changes. These innovative
data processing solutions will allow a live insight of the stress levels
to be provided to individuals with autism and to their caregivers.
Ultimately, this knowledge should allow appropriate intervention,
particularly through the teaching of self-responses in different social
contexts, thus limiting the emergence of disruptive behaviors (Dawson, 2008).
Possibilities are not limited to autism spectrum disorders and many
conditions or working situations should benefit from objective measures
of stress.
Author Contributions
CH, Drafting the article. PC and PRB, Critical revision
of the article. FD, Drafting the article, Final approval of the version
to be published.
Conflict of Interest Statement
The authors declare that the research was conducted in
the absence of any commercial or financial relationships that could be
construed as a potential conflict of interest.
References
Akintola, A. A.,
van de Pol, V., Bimmel, D., Maan, A. C., and van Heemst, D. (2016).
Comparative Analysis of the Equivital EQ02 Lifemonitor with Holter
Ambulatory ECG device for continuous measurement of ECG, heart rate, and
heart rate variability: a validation study for precision and accuracy. Front. Physiol. 7:391. doi: 10.3389/fphys.2016.00391
Boudet, G.,
Walther, G., Courteix, D., Obert, P., Lesourd, B., Pereira, B., et al.
(2017). Paradoxical dissociation between heart rate and heart rate
variability following different modalities of exercise in individuals
with metabolic syndrome: The RESOLVE study. Eur. J. Prevent. Cardiol. 24, 281–296. doi: 10.1177/2047487316679523
Dutheil, F.,
Boudet, G., Perrier, C., Lac, G., Ouchchane, L., Chamoux, A., et al.
(2012). JOBSTRESS study: comparison of heart rate variability in
emergency physicians working a 24-hour shift or a 14-hour night shift–a
randomized trial. Int. J. Cardiol. 158, 322–325. doi: 10.1016/j.ijcard.2012.04.141
Hollocks, M. J.,
Howlin, P., Papadopoulos, A. S., Khondoker, M., and Simonoff, E. (2014).
Differences in HPA-axis and heart rate responsiveness to psychosocial
stress in children with autism spectrum disorders with and without
co-morbid anxiety. Psychoneuroendocrinology 46, 32–45. doi: 10.1016/j.psyneuen.2014.04.004
Malik, M.,
Bigger, J. T., Camm, A. J., Kleiger, R. E., Malliani, A., Moss, A. J.,
et al. (1996). Heart rate variability: standards of measurement,
physiological interpretation and clinical use. Task Force of the
European Society of Cardiology and the North American Society of Pacing
and Electrophysiology. Circulation 93, 1043–1065. doi: 10.1161/01.CIR.93.5.1043
Keywords: stress, anxiety, biomarker, autism, heart rate variability, objective measures
Citation: Hufnagel C, Chambres P, Bertrand PR and Dutheil F (2017) The Need for Objective Measures of Stress in Autism. Front. Psychol. 8:64. doi: 10.3389/fpsyg.2017.00064
Received: 09 November 2016; Accepted: 11 January 2017;
Published: 27 January 2017.
Published: 27 January 2017.
Reviewed by:
Bruno Bonaz, Grenoble Faculty of Medicine and Hospital, France
Alexandra Key, Vanderbilt University Medical Center, USA
Bruno Bonaz, Grenoble Faculty of Medicine and Hospital, France
Alexandra Key, Vanderbilt University Medical Center, USA